You’ve heard the buzz: more peptides, faster results. But is stacking GH secretagogues truly the secret to superior growth? When it comes to growth hormone (GH) support, “stacking” secretagogues sounds enticing; however, the most innovative and budget-friendly strategy is to identify the single agent that best aligns with your goals and physiology. In practice, that usually means trialing sermorelin, tesamorelin, and CJC-1295/ipamorelin individually, tracking benefits, and then deciding whether any stack adds enough incremental value to justify the extra cost.
Vita Bella redefines peptide therapy through clinical precision and personal care. We help you identify the secretagogue that genuinely resonates with your biology. Restore, rebuild, and renew your energy and confidence. Growth isn’t excess; it’s balance perfected through Vita Bella.
Why isn’t stacking GH secretagogues automatically superior?
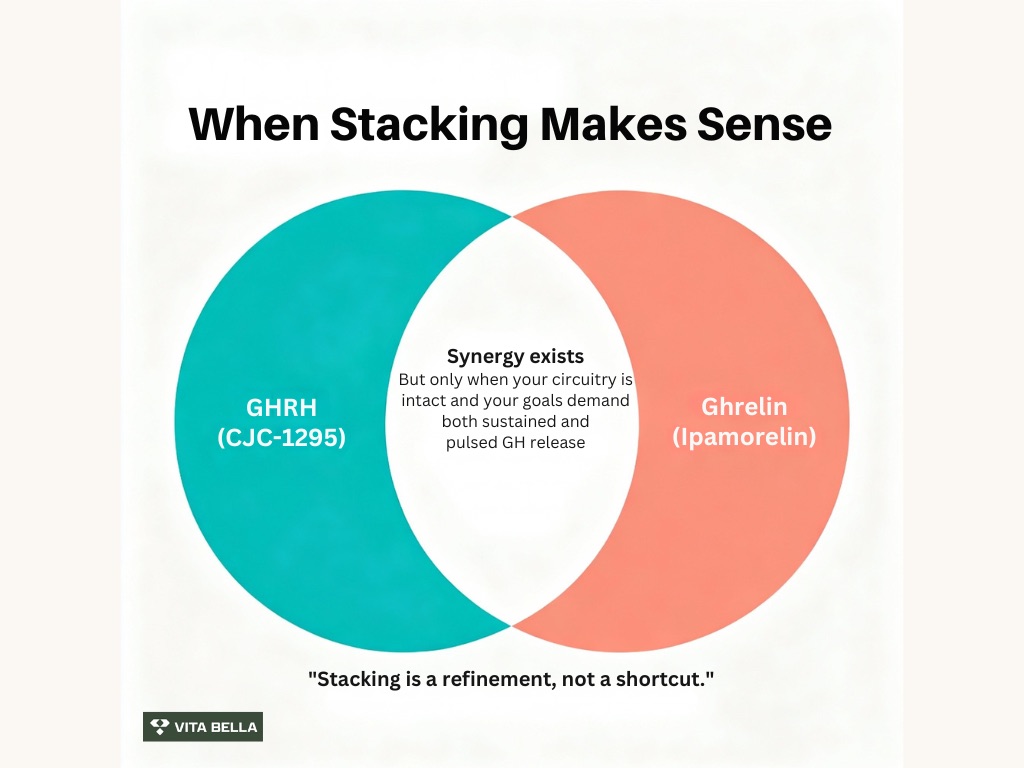
At first glance, combining a GHRH-pathway peptide (e.g., CJC-1295) with a ghrelin-receptor secretagogue (e.g., ipamorelin) seems like an obvious win because the two pathways are complementary; nevertheless, the question is whether the added cost and complexity outperform the right single agent for you.
Human physiology does support synergy between GHRH and ghrelin mimetics under certain conditions, but real-world superiority should be judged against your personal response to each component first. A study1 shows that in patients with hypothalamo-pituitary disconnection, the synergy of GHRH plus GHRP-6 disappeared, clarifying how dual-pathway effects depend on intact circuitry.
Which GH secretagogue works best for you, and how can you find out?
GH biology is highly individual; you’ll get the clearest signal by testing agents separately before you consider a stack. Track sleep, recovery, waist circumference, energy, and (where appropriate) IGF-1 or body-composition metrics over 8–12 weeks. This disciplined approach helps you find your “best responder” and avoid paying for two peptides when one already delivers your outcomes.
Research2 shows that, with a concentration required for half-maximum GH stimulation of 214 nmol/L and a maximal GH production rate of 694 mlU/L/h, ipamorelin induces GH release at all dosage levels. Compared to the PK values, the PD parameters showed more inter-individual variability. Ipamorelin’s dose-response and time-course in healthy volunteers have been mapped with PK/PD modeling, enabling predictable, titratable pulses during individual trials.
The contenders: what each GH secretagogue can do on its own?
GH secretagogues can deliver measurable benefits via the body’s own GH–IGF-1 axis, letting you choose based on data rather than hype. Researchers3 demonstrated that in healthy people, subcutaneous injection of CJC-1295 produced long-lasting, dose-dependent elevations in GH and IGF-I levels. It was also safe and generally well tolerated, especially at dosages of 30 or 60 μg/kg. After several dosages, there was an indication of a cumulative impact.
Sermorelin (GHRH 1-29): physiologic primer
Sermorelin stimulates the pituitary to release GH in a pulsatile manner, supporting natural feedback and typically a favorable tolerability profile. Study4 shows that in pediatrics, sustained increases in height velocity over 12 months and sometimes maintained to 36 months highlight its clinical effectiveness when the goal is gentle, upstream stimulation. The following are the functions where sermorelin can shine:
You want a naturalistic GH rhythm (sleep, recovery, wellness).
You prefer a lighter-touch option before escalating intensity.
You value a cost-conscious first trial to see if physiology alone meets your goals.
Tesamorelin: the body-composition specialist
Tesamorelin is a stabilized GHRH analogue with robust human RCT data for visceral adipose tissue (VAT) reduction, a change tightly linked to metabolic health and waistline improvement. In a pivotal randomized clinical trial5, tesamorelin reduced VAT and also lowered liver fat, underscoring benefits beyond the beltline.
Moreover, an extensive multicenter NEJM study6 in 412 adults with HIV-associated central fat accumulation demonstrated meaningful reductions in VAT and favorable metabolic signals, cementing tesamorelin’s role when selective fat remodeling is the priority. Where tesamorelin can shine:
You prioritize waistline and metabolic improvements.
You want targeted VAT reduction with human RCT support.
You’re comfortable with a daily regimen to maintain effects.
CJC-1295 / Ipamorelin: duration and pulse
CJC-1295 extends GHRH signaling over days, elevating GH 2–10× and IGF-1 for ~9–11 days after dosing in healthy adults; this creates a higher “baseline readiness” for GH release that many people perceive as steadier energy, recovery, and performance support. Ipamorelin, by contrast, delivers brief, controllable GH pulses with minimal cross-activation of other pituitary hormones, ideal when you want on-demand spikes layered onto a sustained background. Where CJC-1295 / ipamorelin can shine:
You want less frequent dosing and a longer effect window.
You respond well to a dual strategy of baseline support (CJC-1295) and timed pulses (ipamorelin).
You’re optimizing training recovery and day-to-day energy.
Is the stacking of GH secretagogues worth it?
Sometimes, but only after you’ve identified your best single agent. If sermorelin already restores sleep and recovery, or tesamorelin delivers the VAT change you want, or CJC-1295 provides the day-to-day lift you feel, adding a second peptide may give diminishing returns relative to cost. Conversely, suppose your best responder still leaves a gap (e.g., you want both sustained energy and sharper workout-day pulses).
In that case, a CJC-1295 + ipamorelin stack can be rational because physiology supports complementary mechanisms. (Human data1 demonstrating loss of GHRH+GHRP synergy after hypothalamo-pituitary disconnection clarifies that dual-pathway effects are real when circuitry is intact.)
Don’t Overload, Optimize secretagogue with Vita Bella.
More peptides don’t always mean more progress. Over-stacking can overwhelm your system, wasting effort and resources. The root cause is an imbalance in a disrupted GH–IGF-1 axis that can’t respond appropriately. Your body needs a more intelligent, targeted solution to perform and recover optimally. Sustainable results come from restoring balance, not pushing harder.
At Vita Bella, we optimize growth through precision, not excess. Our peptide specialists tailor treatment to your unique physiology, helping you find the perfect secretagogue for your goals. Experience higher energy, better sleep, and visible results all without unnecessary stacking. Choose more innovative science, your transformation begins with Vita Bella.
FAQs
Can stacking multiple GH secretagogues deliver faster or stronger results?
Yes, stacking can sometimes enhance GH release by combining different receptor pathways, but more isn’t always better. Excess peptides may overstimulate your system, leading to diminishing returns. The most effective results come from precision, identifying which peptide, such as Sermorelin, Tesamorelin, or CJC-1295/Ipamorelin, aligns best with your physiology and goals.
Is it necessary to use multiple peptides to see noticeable benefits?
No, most individuals experience measurable improvements using a single well-matched GH secretagogue. When chosen correctly, one peptide can effectively enhance energy, body composition, and recovery. Over-stacking increases cost and complexity without guaranteed synergy. Personalized, evidence-based selection, as practiced at Vita Bella, delivers smarter, sustainable growth hormone optimization.
Does stacking GH secretagogues affect natural hormone balance?
Yes, excessive stacking can disrupt natural GH feedback loops, potentially dulling the body’s rhythm over time. Human physiology thrives on pulsatility, not constant stimulation. A balanced approach guided by clinical insight helps maintain your GH–IGF-1 axis, allowing peptides to work harmoniously without compromising your body’s natural hormonal balance.
Is it better to find one peptide that works for me rather than stacking several?
Yes, finding your ideal single peptide is both physiologically more innovative and financially efficient. Each person responds differently to GH secretagogues, and precision consistently outperforms quantity. At Vita Bella, we help you test and identify your best-fit peptide so you can achieve consistent, visible results without unnecessary stacking or expense.
References:
Popovic, V., Damjanovic, S., Micic, D., Djurovic, M., Dieguez, C., & Casanueva, F. F. (1995). Blocked growth hormone-releasing peptide (GHRP-6)-induced GH secretion and absence of the synergic action of GHRP-6 plus GH-releasing hormone in patients with hypothalamopituitary disconnection: Evidence that GHRP-6 main action is exerted at the hypothalamic level. Neuroendocrinology, 61(4), 445–452. https://doi.org/10.1159/000126868
Gobburu, J. V. S., Agersø, H., Jusko, W. J., & Ynddal, L. (1999). Pharmacokinetic-pharmacodynamic modeling of ipamorelin, a growth hormone releasing peptide, in human volunteers. Pharmaceutical Research, 16(9), 1412-1416. https://doi.org/10.1023/A:1018955126402
Teichman, S. L., Neale, A., Lawrence, B., Gagnon, C., Castaigne, J.-P., & Frohman, L. A. (2006). Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. The Journal of Clinical Endocrinology & Metabolism, 91(3), 799–805. https://doi.org/10.1210/jc.2005-1536
Prakash, A., & Goa, K. L. (1999). Sermorelin: A review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency. BioDrugs, 12(2), 139-157. https://doi.org/10.2165/00063030-199912020-00007
Stanley, T. L., Feldpausch, M. N., Oh, J., Branch, K. L., Lee, H., Torriani, M., & Grinspoon, S. K. (2014). Effect of tesamorelin on visceral fat and liver fat in HIV-infected patients with abdominal fat accumulation: A randomized clinical trial. JAMA, 312(4), 380–389. https://doi.org/10.1001/jama.2014.8334